Patient K., 35, complained of absence of incisive tooth and insufficient aesthetical criteria of dental bridge that substituted the lost tooth. The tooth had been lost resulting from trauma more than 5 years ago, for which reason the patient was performed the osteoplasty with bone autoblock, taken from the area of mandibular ramus bone.
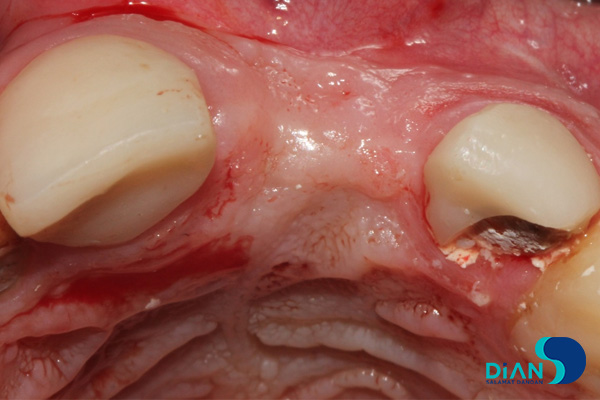
Observed: plastic dental bridge covering the incisors on a maxillary bone is detected during the examination of oral cavity. In the area of the tooth 2.1 there is an intermediate part of the bridge with a bad attachment to alveolar mucosa, what makes an effect of interspace between crown and gum difficult for cleaning.

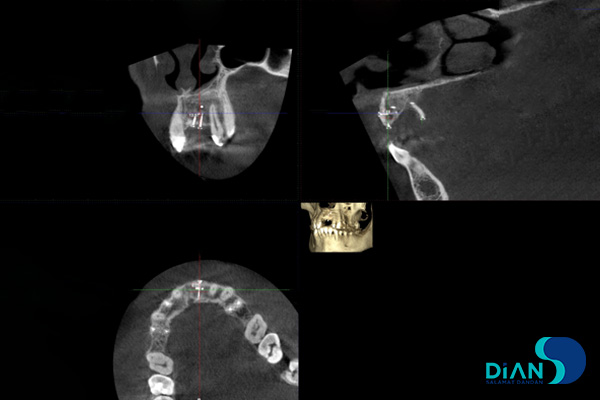
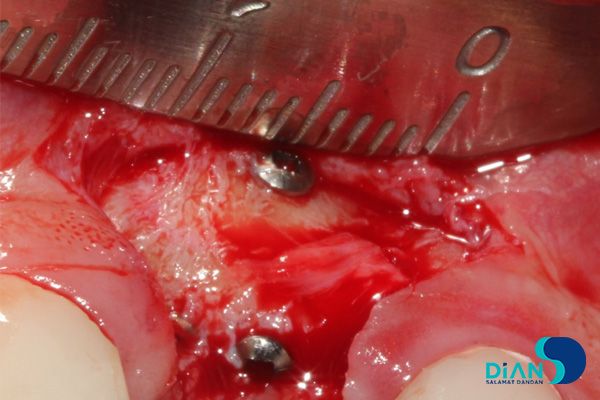
In the CBCT tomography results there are traces of an earlier osteoplasty in the area of tooth 2.1 in the type of foreign object, its form appropriate to the titanium micro screw for the fixation of bone blocks.
The decision was taken on the implantation with immediate loading in the area of missing tooth 2.1. The implant Bio3 Progressive with conical form and aggressive thread was chosen with account of the topography of the defect (maxillary bone), bone density (D2-D3), and planned immediate loading to obtain high primary stability rate of relatively soft bone.
Operation Process
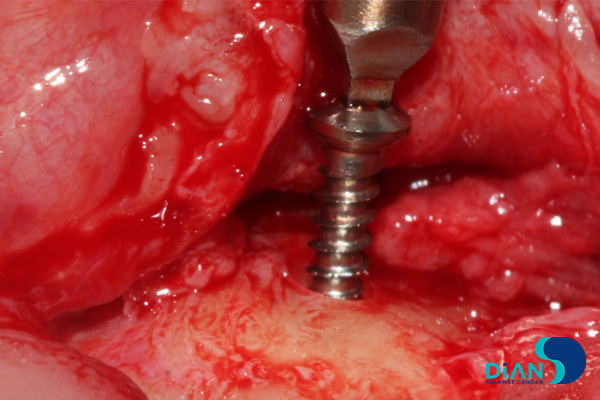
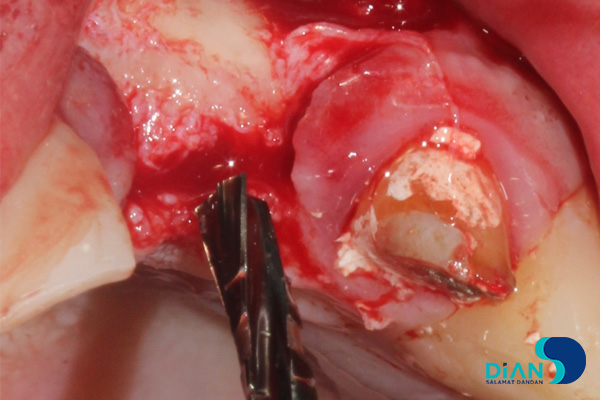
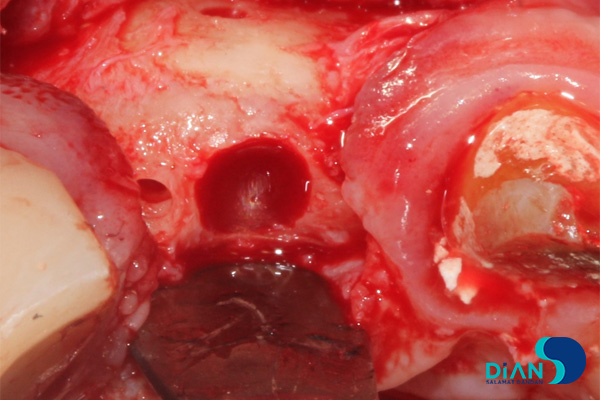
After the antiseptic preparation of the operative field with Betadine solution, under local anesthesia with Ultracain D-S a full cut of mucous membrane of alveolar bone’s facial surface was made in the area of teeth 2.1, cortical plate was skeletonized with raspatory, screws fixing transplant were found and removed.
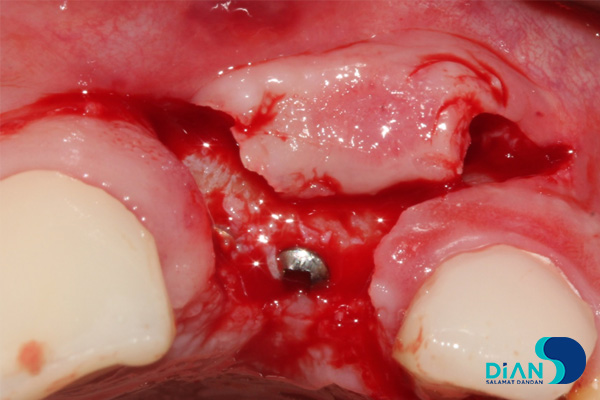
Bone cavity for the future implant was made through series of osteotomy 2 mm deeper of its height, paying attention to the position and axis of adjacent teeth.
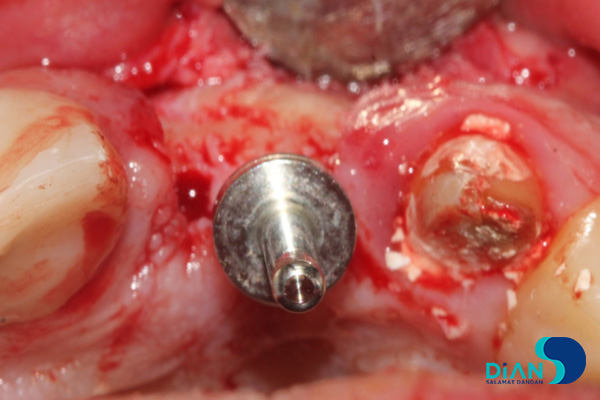
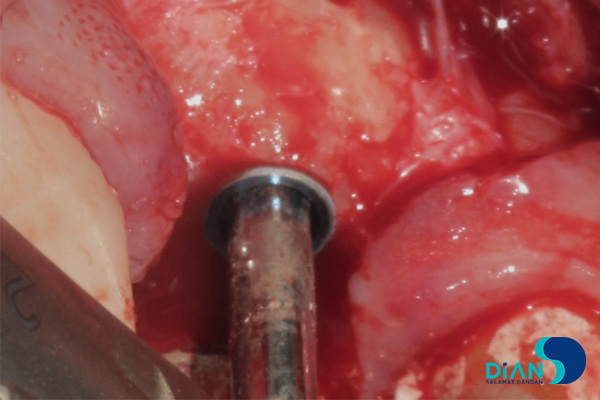
Incomplete drilling protocol was made during the drilling with the objective to obtain a high rate of primary stability and with a factual bone density taken into account. Cavity of cortical plate was extended with the profile drill. Implant cavity was irrigated with sterile normal saline and Dioxydin solution, bone remnants were removed. Implant Progressive 3.8/10 was integrated into the bone cavity subcrestally and fixated with the force of 30-40N.
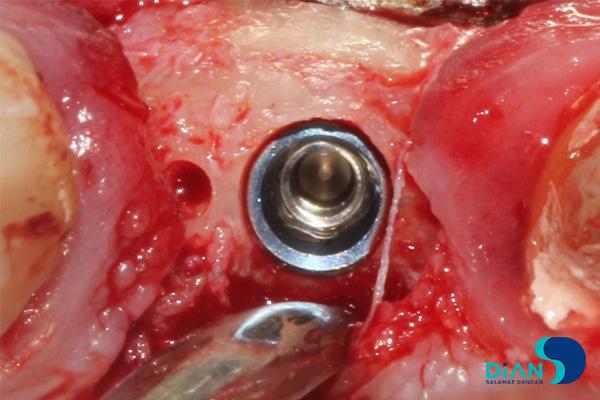

The direct titanium abutment was fixated in the implant. Control radiography of the integrated implant was performed.

Temporary crown was formed and fixated with the force of 15N.

It is recommended to debride mouth cavity within the postoperative period. The Bio3 Implant Care Foam, preventive antibiotics and anesthetic therapy correspond the established norms.
Reference
Kobyakov Aleksandr Vladimirovich, N.I. Pirogov Vinnitsa National Medical University